
The multi-luting concept: a new approach to facilitate the adhesive luting of multiple indirect restorations

Bonded indirect restorations can be difficult to lute in an accurate position due to the lack of preparation geometry. Furthermore, while the use of a rubberdam has been proven to be the best technique for providing the most efficient conditions for adhesive luting, its use often requires the use of secondary clamps, which do not allow the operator to lute more than two prosthetic pieces at the same time. The multi-luting concept is a pragmatic approach that offers the possibility to deliver several, if not all restorations, to be bonded at the same time, thus ensuring their correct positioning.
Authors:
-
David Gerdolle DMD MS, Private Practice, Montreux, Switzerland
-
Stephane Browet DMD, Private Practice, Brussels, Belgium
-
Marco Gresnigt DMD PhD, Associate Professor, Department of Restorative Dentistry, University Medical Center Groningen, Center for Dentistry and Oral Hygiene, University of Groningen, The Netherlands.
Keys words: Adhesion, prosthodontics, isolation, adhesive, luting, ceramic, veneer, onlay, inlay
Résumé
Le concept du collage multiple : une nouvelle approche pour faciliter le scellement adhésif de multiples restaurations indirectes en un temps opératoire.
Les restaurations indirectes collées peuvent être difficiles à placer dans une position précise en raison du manque de géométrie de la préparation. En outre, s'il a été prouvé que l'utilisation de la digue est la technique pour un scellement adhésif de qualité, son utilisation va souvent de pair avec l'utilisation de clamps secondaires, qui ne permettent pas à l'opérateur de sceller plus de deux pièces prothétiques en même temps. Le concept du collage multiple est une approche pragmatique qui offre la possibilité de cimenter plusieurs, voire tous les composants prothétiques à coller en même temps, assurant ainsi leur positionnement correct.
Introduction
Over the last 30 years, restorative dentistry has fundamentally changed, emulating structurally and visually the natural tooth. (BAZOS & MAGNE 2011 & 2014). In particular, the use of a composite resin bonding material, capable of adhering to dental tissue as well as restorative materials, allows for less invasive dental preparations, as no geometric retention is required (EDELHOFF & SORENSEN 2002). In addition, prosthetic materials have better mechanical properties when the design of the dental preparation features only smooth, rounded surfaces (GUESS & COLL 2013, POLITANO & COLL 2018, BLUNCK U & COLL 2020). This conservative approach is beneficial in terms of biology, as it allows for more invasive treatment solutions in the future, which is more favorable as the life expectancy of our patients increases.
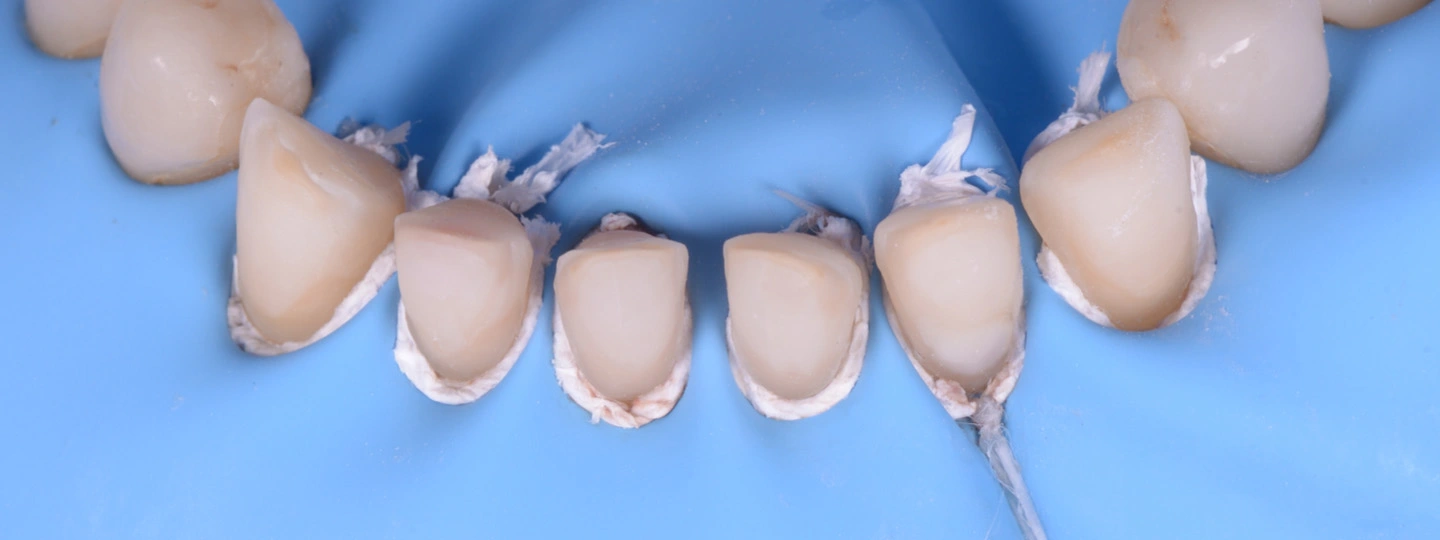
Nevertheless, these non-geometric preparations complicate accurate positioning of the indirect restorations, particularly when several restorations need to be inserted (PEREIRA SILVA & COLL 2021). In addition, the use of absolute isolation with a rubber dam during the bonding procedure has been shown to result in greater bond strength (PASHLEY & COLL 1982, ELKASSAS & ARAFA 2016, FALACHO & COLL. 2022). However, the use of a rubberdam isolation can also complicate the precise positioning of the restorations to be luted. It may require the use of secondary clamps to manage good access to the margins of the preparations, particularly in the aesthetic zone (GERDOLLE & BROWET 2019). As a result, the insertion of more than two restorations at the same time becomes practically impossible (Figure 1); Considering also that the prosthetic parts must be held under pressure when light curing is initiated (CHIEFFI & COLL 2007), it is easy to understand how mismatches and/or inaccurate positioning of final restorations can occur.
In a previous publication (GERDOLLE & COLL. 2022), an innovative luting technique was presented as a means of improving the longevity of bonded indirect restorations by minimizing margin finishing procedures that can roughen the surface of the bonding composite, leading to increased plaque accumulation and premature ageing (PAOLANTONIO & COLL 2004, PAULO SILVA & COLL 2021). This approach is based on three major principles which are the use of isolation with rubber dam, the use of preheated restorative composites as a bonding agent and the use of a selective light curing technique. The aim of this article is to demonstrate the additional advantages of such a concept by facilitating and securing the positioning of several, or even all, indirect restorations to be bonded at the same time, under absolute rubber dam isolation.


Isolating without using secondary clamps
Multiple and simultaneous luting requires the isolation to meet certain specific criteria (BROWET & GERDOLLE 2017):
1. Quadrant isolation. At least one tooth distal of the most distal prepared tooth must be included in the isolation field.
2. Anchorage clamps are generally used to resist the tension of the rubber sheet distal, as well as to open access to the most distal tooth to be restored. A narrow wingless clamp is often preferred for the purpose, in order to avoid any interference with the most distal prosthetic part (Figure 2).
3. On the other teeth in the quadrant, which includes all the prepared teeth, retraction of the gingiva should allow all the margins of the preparations to be exposed. This makes it possible to check the exact fit of each restoration and does expose the margins sufficiently to polish them after polymerization. In the anterior area especially, the scalloped anatomy of the gingiva can make it difficult to position and stabilize the rubber beyond the vestibular zenith of the preparation (Figure 1).
4. One option is to push and invert the rubber sheet into the sulcus using a double ligature that can be tightened with one hand (Video 1). The operator can then guide the rubber into the sulcus with a small spatula using his second hand. Once the floss ligature has been tightened with a second knot, it can be attached to the frame to ensure slightly greater retraction (Figure 3). If necessary, Teflon tape can be inserted on top of the floss ligature, between the rubber and the root, to provide additional retraction (Figure 4). The final quality of the isolation is defined when all the prosthetic parts can be inserted at the same time with a passive fit, in exactly the same way as they were positioned during the initial try in session (Figure 5). The authors' preference goes for a Teflon strip to provide both vertical and horizontal retraction, placed over a double ligature whose knot has been slid onto the palatal side (Figure 6).
5. Another option would be to place a secondary clamp on the tooth before placing the ligature. Acting as two spatulas (one palatal and one buccal), the prongs of the clamp can then guide the ligature into the sulcus. Once the tightening ensured with a second knot, the clamp can be removed and the retraction can be improved with Teflon tape, if necessary (Figure 7).
The same procedure should be repeated on each prepared tooth.









Luting all simultaneously
In an ideal world, one would love to be able to maintain firm pressure on all the parts to be bonded at the same time during light-curing. Unfortunately, this is impossible to achieve in practice. The fundamental and basic idea is therefore to insert all the prosthetic parts at the same time, so that their precise positioning can be ensured both by the shape of the preparations and by the proximal contact surfaces. Intuitively, the choice of a luting composite resin should be based on a low-viscosity material that offers no resistance to the insertion of the prosthetic element and allows it to be fully seated. However, the consequence of a very fluid consistency is the lack of stability of the parts and the difficulty in correctly removing excess before light-curing. To overcome the latter pitfall, some authors have proposed using a brief flash of light-curing (of the order of one second), to place the fluid composite in a so-called 'gel' phase, enabling excesses to be easily removed in the same way as a conventional sealing cement (CHEN & COLL. 2016, GAILE & COLL .2022). Although the idea is attractive in theory, in practice this procedure seriously impairs the quality of the prosthetic seal, by tearing off a variable quantity of material at the margin (NAVES & COLL. 2020). In contrast, adhesive luting using a viscous restorative composite, introduced as early as 1995 (BESEK & COLL. 1995), offers undeniable clinical advantages, such as remarkable stability of the prosthetic parts before light-curing, improved biomechanical properties, superior wear resistance and, above all, easy removal of excess material (SCHULTE & COLL. 2005, KRAMER & FRANKENBERGER 2005, KRAMER & COLL 2009). In addition, recent papers have demonstrated their ability to have higher bond strength and longevity in vitro (KAMAYEMA & COLL. 2015, GOLDBERG & COLL 2016, GRESNIGT & COLL. 2017) and in vivo (GRESNIGT & COLL. 2019, VAN DER BREEMER & COLL. 2021). In the end, choosing a low or high viscosity will in all cases ensure a quality bond; the ultimate criterion of choice thus remaining ease of clinical application.
If a high viscosity is chosen, the restorative composite, preferably packaged in compules, should be preheated at between 40 and 60°C for a few minutes prior to assembly, in order to lower its viscosity, following the recommendation of each manufacturer. The creamy consistency thus obtained allows easy insertion under firm manual pressure (Video 2). With simultaneous insertion, the parts are self-positioning beyond the simple manual guidance provided by the operator. The viscous consistency of the luting composite resin is beneficial at this stage, as the prosthetic parts are more stable in position than when fluid luting products are used. Some authors recommend the use of ultrasound to assist insertion and thus reduce joint thickness (FALACHO AND COLL. 2021). However, having applied both insertion techniques without noticing any clinical differences (particularly in terms of occlusion), the authors currently prefer not to use ultrasound-assisted insertion, as it is difficult to assess its impact on the microstructure of the prosthetic material. Once the initial insertion has been completed, the largest excesses are immediately removed and further manual pressure is applied to check that the restoration is fully seated.
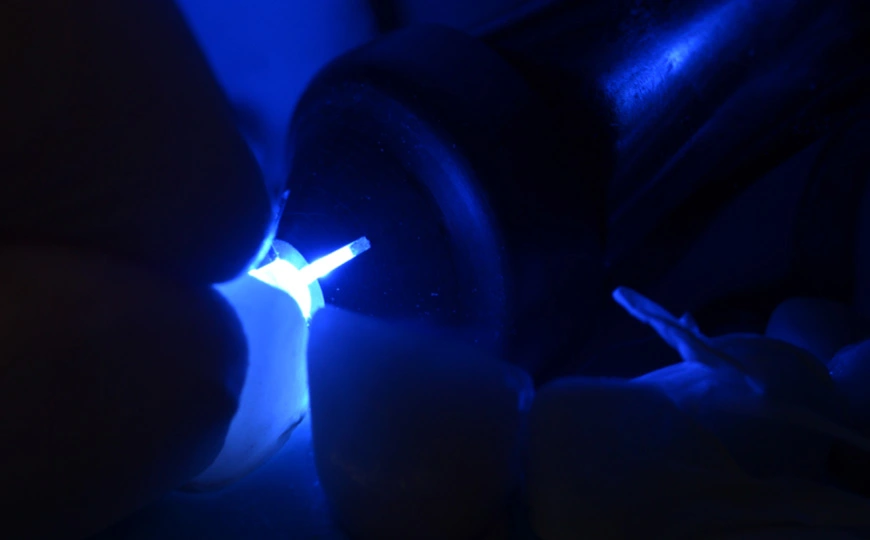
Once the biggest excesses have been removed, the most accessible part of the margins of each tooth to be restored is then selected to be smoothen and perfectly finished before polymerization, using a brush slightly impregnated of hydrophobic resin (GERDOLLE & COLL 2022). For anterior veneers, the palatal margin is generally selected for the purpose. Then, maintaining the prosthetic pieces two by two, a selective polymerization is applied though a collimation tip (Valo Curing collimating lens, Ultradent™) on the distal part of the most distal element for 3 to 5s under a low power (500mW/cm2 or less) (figure 8). The operator then moves one tooth mesial and repeats the same procedure from one to the next tooth. So that all restorations are now blocked into their final position without the less accessible of the margins being polymerized. This gives the possibility to the operator to eliminate further residual excesses and then to smoothen these uncured margins using the same brush slightly impregnated of modeling resin (Video 2 & 3).
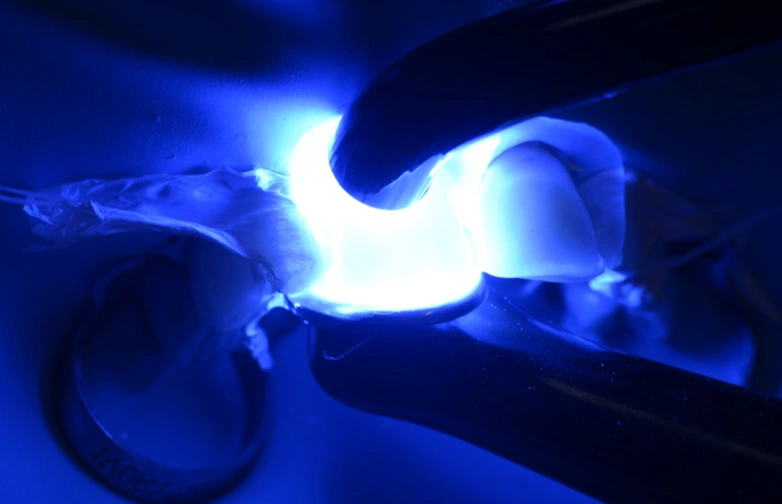
When all the margins look smooth and free of luting composite excesses, a second polymerization is performed. All the surfaces of the teeth are thus light-cured for about 20s, at low to moderate power (500 to 1000mW/cm2) under air cooling (JUNG & COLL 2006) (Figure 9).
At this stage the margins can be refined, preferably avoiding any diamond instruments that would roughen their surfaces and complicate or even prevent a satisfactory final polishing. A number 12 blade is most likely used for the purpose (Video 3).
The final polishing is then carefully proceeded using silicone points and discs. Finally, further light-polymerization is achieved at high power (above 1000mW/cm2), using preferably two curing units for the irradiance to be more uniform and for about 1 to 2 minutes per tooth, under glycerin gel and/or constant water cooling (PRICE 2017, DE KUIJPER 2021) (Video 3).
Conclusion
A major criteria for success when bonding indirect restorations is to be able to achieve an accurate positioning under absolute isolation. Using secondary clamps to retract the gum and push the rubber sheet beyond the margin, does force the operator to lute the indirect restorations one by one or two by two, when two clamps are used for the purpose. The multi-luting concept allows a simultaneous and accurate insertion of all the restorations by achieving an absolute isolation without using clamps though. Furthermore, by using viscous pre-heated restorative composite as a luting agent and by polymerizing selectively each tooth, it gives the ability for the operator to achieve, with no working time restriction, a smooth finishing of the margins, leading to a better longevity of the restorations.
Videos
Double ligature for veneer cementation
Onlay Veneer cementation
Veneer cementation
Bibliography
BAZOS P, MAGNE P: Bio-emulation: biomimetically emulating nature utilizing a histo-anatomic approach; structural analysis. Eur J Esthet Dent. Spring;6(1):8-19 (2011)
BAZOS P, MAGNE P: Bio-Emulation: biomimetically emulating nature utilizing a histoanatomic approach; visual synthesis. Int J Esthet Dent, Autumn;9(3):330-52 (2014)
BESEK M, MÖRMANN WH, PERSI C, LUTZ F: The curing of composites under Cerec inlays. Schweiz Monatsschr Zahnmed 105(9):1123-8 (1995)
BLUNCK U, FISCHER S, HAJTÓ J, FREI S, FRANKENBERGER R: Ceramic laminate veneers: effect of preparation design and ceramic thickness on fracture resistance and marginal quality in vitro. Clin Oral Investig. Aug;24(8):2745-54 (2020)
BROWET S, GERDOLLE D: Precision and security in restorative dentistry: the synergy of isolation and magnification. Int J Esthet Dent 12(2):172-185 (2017)
CHEN L, SUH BI, GLEAVE C, CHOI WJ, HYUN J, NAM J: Effects of light-, self-, and tack-curing on degree of conversion and physical strength of dual-cure resin cements, Am J Dent Apr;29(2):67-70 (2016).
CHIEFFI N, CHERSONI S, PAPACCHINI F, VANO M, GORACCI C, DAVIDSON CL, TAY FR, FERRARI M: The effect of application sustained seating pressure on adhesive luting procedure. Dent Mater. Feb;23(2):159-64 (2007)
DE KUIJPER M, ONG Y, GERRITSEN T, CUNE MS, GRESNIGT MMM: Influence of the ceramic translucency on the relative degree of conversion of a direct composite and dual-curing resin cement through lithium disilicate onlays and endocrowns. J Mech Behav Biomed Mater Oct;122:104662 (2021)
EDELHOFF D, SORENSEN JA: Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. May;87(5):503-9 (2002)
ELKASSAS D, ARAFA A: Assessment of post-contamination treatments affecting different bonding stages to dentin, Eur. J. Dent. 10:327–332 (2016)
FALACHO RI, MARQUES JA, PALMA PJ, ROSEIRO L, CARAMELO F, RAMOS JC, GUERRA F, BLATZ MB: Luting indirect restorations with resin cements versus composite resins: Effects of preheating and ultrasound energy on film thickness. J Esthet Restor Dent Dec 13 (2021)
FALACHO RI, MARQUES JA, PALMA PJ, ROSEIRO L, CARAMELO F, RAMOS JC, GUERRA F, BLATZ MB: Luting indirect restorations with resin cements versus composite resins: Effects of preheating and ultrasound energy on film thickness.
J Esthet Restor Dent. Jun;34(4):641-649 (2022)
GAILE M, PAPIA E, ZALITE V, LOCS J, SOBOLEVA U: Resin Cement Residue Removal Techniques: In Vitro Analysis of Marginal Defects and Discoloration Intensity Using Micro-CT and Stereomicroscopy. Dent J (Basel). Apr 1;10(4):55 (2022)
GERDOLLE D, BROWET S: The secrets of isolation in the cervical area. Swiss Dent J May 13;129(5):371-379 (2019)
GERDOLLE D, BROWET S, GRESNIGT M: the perennity of indirect bonded restorations: the “no-finishing concept”. Swiss Dent J. Jul 11;132(7-8):499-504 (2022)
GOLDBERG J, GUTH JF, MAGNE P: Accelerated fatigue resistance of thick CAD/CAM composite resin overlays bonded with light- and dual-polymerizing luting resins. J Adhes Dent 18:341–348 (2016)
GRESNIGT MMM, OZCAN M, CARVALHO M, LAZARI P, CUNE MS, RAZAVI P, MAGNE P: Effect of luting agent on the load to failure and accelerated-fatigue resistance of lithium disilicate laminate veneers. Dent Mater 33:1392–1401 (2017)
GRESNIGT MMM, CUNE MS, SCHUITEMAKER J, VAN DER MADE SAM, MEISBERGER EW, MAGNE P, ÖZCAN M: Performance of ceramic laminate veneers with immediate dentine sealing: An 11 year prospective clinical trial., Dent. Mater. 35 :1042–1052 (2019)
GUESS PC, SCHULTHEIS S, WOLKEWITZ M, ZHANG Y, STRUB JR: Influence of preparation design and ceramic thicknesses on fracture resistance and failure modes of premolar partial coverage restorations.
J Prosthet Dent. Oct;110(4):264-73 (2013)
JUNG H, FRIEDL KH, HILLER KA, FURCH H, BERNHART S, SCHMALZ G: Polymerization efficiency of different photocuring units through ceramic discs. Oper Dent 31:68–77 (2006)
KAMEYAMA A, BONROY K, ELSEN C, LUHRS AK, SUYAMA Y, PEUMANS M, VAN MEERBEEK B, DE MUNCK J: Luting of CAD/CAM ceramic inlays: direct composite versus dual-cure luting cement. Biomed Mater Eng 25:279–288 (2015)
KRAMER N, FRANKENBERGER R: Clinical performance of bonded leucite-reinforced glass ceramic inlays and onlays after eight years. Dent Mater 21:262–271 (2005)
KRAMER N, REINELT C, RICHTER G, FRANKENBERGER R: Four-year clinical performance and marginal analysis of pressed glass ceramic inlays luted with ormocer restorative vs. conventional luting composite. J Dent 37:813–819 (2009)
NAVES LZ, GERDOLLE DA, DE ANDRADE OS, MARKUS MARIA GRESNIGT M: Seeing is believing? When scanning electron microscopy (SEM) meets clinical dentistry: The replica technique. Microsc Res Tech Sep;83(9):1118-1123 (2020)
PASHLEY DH, NELSON R, KEPLER EE: The Effects of Plasma and Salivary Constituents on Dentin Permeability, J. Dent. Res. 61 978–981 (1982)
POLITANO G, VAN MEERBEEK B, PEUMANS MJ: Nonretentive Bonded Ceramic Partial Crowns: Concept and Simplified Protocol for Long-lasting Dental Restorations.
Adhes Dent. 20(6):495-510 (2018)
PAOLANTONIO M, DERCOLE S, PERINETTI G, TRIPODI D, CATAMO G, SERRA E, BRUÈ C, PICCOLOMINI R: Clinical and microbiological effects of different restorative materials on the periodontal tissues adjacent to subgingival class V restorations. J Clin Periodontol Mar;31(3):200-207 (2004)
PAULO SILVA J, COELHO A, PAULA A, AMARO I, SARAIVA J, MARQUES FERREIRA M, MARTO CM, CARRILHO E: The Influence of Irrigation during the Finishing and Polishing of Composite Resin Restorations—A Systematic Review of In Vitro Studies. Materials (Basel) Mar 29;14(7):1675 (2021)
PRICE RBT: Light Curing in Dentistry. Dent Clin North Am Oct;61(4):751-778 (2017)
SCHULTE AG, VOCKLER A, REINHARDT R: Longevity of ceramic inlays and onlays luted with a solely light-curing composite resin. J Dent May;33(5):433-42 (2005)
SILVA BP, MAHN ARTEAGA G, MAHN E: Predictable 3D guided adhesive bonding of porcelain veneers using 3D printed trays. J Esthet Restor Dent. Jul;33(5):692-701 (2021)
VAN DEN BREEMER CRG, BUIJS GJ, CUNE MS, ÖZCAN M, KERDIJK W, VAN DER MADE S, GRESNIGT MMM: Prospective clinical evaluation of 765 partial glass-ceramic posterior restorations luted using photo-polymerized resin composite in conjunction with immediate dentin sealing. Clin Oral Investig Mar;25(3):1463-1473 (2021)
Bibliography
![]()